From Gd-160 to Tb-161: Revolutionizing Theranostic Applications in Nuclear Medicine
BY Tao, Published Dec 28, 2025
From the early days of Iodine-131 to the recent dominance of Lutetium-177 (177Lu), each generation of isotopes has pushed the boundaries of what is clinically possible. However, as we stand here in late 2025, reflecting on the breakthroughs of the past year, it is increasingly clear that we are on the cusp of a new revolution. The torch is being passed from the well-established Lutetium-177 to a nuclide that offers unprecedented precision for targeting micrometastases: Terbium-161 (Tb-161). China Isotope Development Co.,Ltd ,as a emerging Isotope supplier, was supplying Gadolinium-160 (Gd-160) to serve Researches & Institues step by step , gaining their trust ranging from its quality / price / delivery. Today, I will take you through the intricate journey from the raw material, enriched Gadolinium-160 (), to the therapeutic powerhouse that is Terbium-161. We will explore why this transition is not just a scientific curiosity but a clinical necessity.
The Foundation: Why Gadolinium-160 Matters
To understand the value of Terbium-161, we must first appreciate its origin. High-purity isotope production is an art form as much as it is a science, and it begins with the target material. For , that starting point is Gadolinium-160.
The Challenge of Neutron Capture
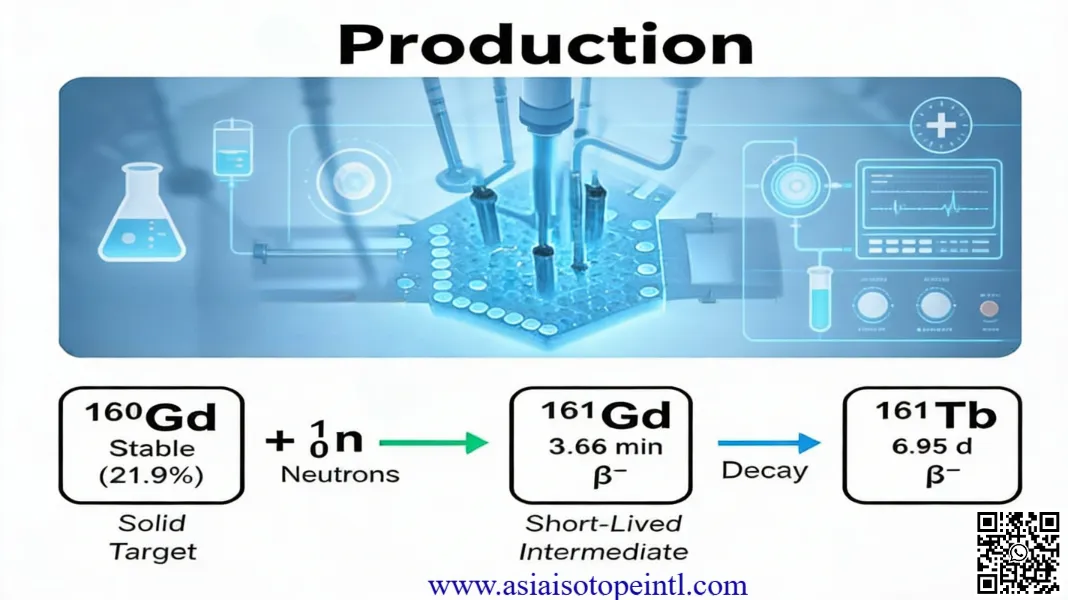
Producing high-specific-activity radionuclides requires a clean nuclear reaction. We utilize the neutron capture pathway: 160Gd(𝑛,𝛾)161Gd. This intermediate isotope, Gadolinium-161, has a short half-life of roughly 3.66 minutes and rapidly decays via beta emission into our desired product, Terbium-161 .
However, “natural” gadolinium is a nightmare for this process. It contains isotopes like Gd-155 and Gd-157, which have colossal neutron capture cross-sections (61,000 and 254,000 barns, respectively) . If you were to put natural gadolinium in a reactor, these isotopes would act as “neutron poisons,” absorbing the neutrons meant for Gd-160 and killing the efficiency of the reaction.
This is why enriched Gd- is non-negotiable. As experts, we demand enrichment levels often exceeding 98% to ensure that the neutron flux is utilized efficiently and to minimize radiochemical impurities that complicate downstream separation. The purity of the input determines the quality of the output.
The Star: Terbium-161 vs. Lutetium-177
For years, Lutetium-177 has been the gold standard for treating neuroendocrine tumors and prostate cancer. So, why fix what isn’t broken? The answer lies in the physics of “micro-dosimetry.”
The Power of Auger Electrons
Both Lu- and Tb- are radiolanthanides with similar chemical properties, meaning we can often use the same chelators (like DOTA) to attach them to drug molecules . They also both emit beta particles (𝛽−) that travel a few millimeters in tissue to kill tumor cells.
But here is the critical difference: Terbium-161 possesses a “hidden weapon” that Lutetium lacks.
In addition to beta particles, Tb- emits a significantly higher number of conversion electrons and Auger electrons.
- Beta particles are like long-range artillery; they are great for bulk tumors but can sometimes overshoot very small clusters of cancer cells.
- Auger electrons are like daggers; they have extremely low energy (often <50 keV) and travel incredibly short distances (sub-micrometer to micrometer range), often less than the width of a single cell .
While Lu- emits very few of these low-energy electrons, Tb- emits an abundance. Specifically, Tb- releases approximately 2.4 times more energy per decay into these small volumes compared to Lu-. This means that if a cancer cell has internalized the radioactive drug, the Auger electrons from Terbium-161 will deliver a lethal dose directly to the cell’s DNA and membrane, while sparing the healthy tissue just a few cells away.
Comparison of Key Parameters
| Feature | Lutetium-177 (Lu-) | Terbium-161 (Tb-) | Clinical Impact |
|---|---|---|---|
| Half-Life | 6.65 days | 6.89 days | Identical logistics for shipping and patient scheduling . |
| Primary Decay | Beta (𝛽−) | Beta (𝛽−) | Both effective for larger tumors. |
| Gamma Emission | 113 keV, 208 keV | 49 keV, 75 keV | Both allow for SPECT imaging to monitor treatment distribution . |
| Auger/Conversion | Low Yield | High Yield | Tb- is far superior for micrometastases and single-cell killing . |
| Production | Established | Scaling Up | Tb- supply chains are maturing rapidly in 2026. |
The Art of Separation: Purifying the Product
Once the enriched Gd-160 target has been irradiated, we are left with a mixture of the target material, the desired Tb-, and stable Dysprosium-161 (Dy-), which is the decay product of Terbium.
Separating adjacent lanthanides (like Gadolinium, Terbium, and Dysprosium) is notoriously difficult because their chemical behaviors are almost identical. In my lab, we utilize advanced chromatography techniques—specifically cation exchange and extraction chromatography (using resins like LN or DGA) .
The process generally involves two stages:
- Bulk Separation: Removing the massive amount of valuable enriched Gadolinium target (which we recycle) from the microscopic amount of Terbium produced.
- Fine Purification: Removing trace contaminants and the stable Dy- to ensure “No-Carrier-Added” (NCA) specific activity. High specific activity is crucial because we want every receptor on a cancer cell to be occupied by a radioactive atom that kills it, not a stable atom that does nothing .
Clinical Frontiers: 2025 and Beyond
The theoretical advantages of Auger electrons have now translated into clinical reality. As we review the data from late 2024 and 2025, the results are compelling.
Prostate Cancer (PSMA)
In the realm of Metastatic Castration-Resistant Prostate Cancer (mCRPC), we have seen trials like the study of Tb--PSMA-I&T. Early phase results have shown that Tb- can deliver high absorbed doses to tumors with manageable toxicity . More importantly, for patients with “micrometastatic” disease—tiny spread that often escapes Lutetium therapy—Terbium’s Auger electrons appear to offer better control .
Neuroendocrine Tumors (NETs)
Similarly, for NETs treated with DOTATATE, the switch to Terbium is being explored to reduce relapse rates. The hypothesis is simple: Lutetium shrinks the big tumors, but Terbium might be required to “mop up” the microscopic residue that causes recurrence.
Strategic Outlook
The transition from Gd-160 to Tb-161 is not just a replacement; it is an evolution. We are moving from “hitting the target” to “obliterating the target with precision.” For pharmaceutical companies and clinical researchers, the supply chain of enriched Gd- and the availability of GMP-grade Tb- are the critical bottlenecks that are finally being resolved this year.
As we look toward 2026, I anticipate Tb- will sit alongside Lu- in the radiopharmacy—not necessarily replacing it entirely, but becoming the agent of choice for disseminated, small-volume disease where precision is paramount.
Would you like a deeper dive into any specific technical parameters or applications?
As an industry leader focused in isotope products, our goal is to support our customers by keeping them at the forefront of their industries. We’re here to help with any questions you might have so you can transform your ideas into reality, and tackle those big science challenges.
Get free consultant, our experts are ready to serve.
(Follow up our update articles on www.asiaisotopeintl.com or send your comments to tao.hu@asiaisotope.com for further communications)