Gadolinium-160: The Essential Precursor for Terbium-161 Production in Targeted Cancer Radiotherapy
BY Tao, Published Dec 28, 2025
Terbium-161 (Tb-161) is emerging as one of the most promising “next-step” therapeutic radionuclides for targeted radionuclide therapy (also called targeted radiotherapy or radioligand therapy) because it behaves chemically like the widely used Lutetium-177 (Lu-177), yet delivers additional ultra-short-range electron dose that may improve tumor cell kill—especially in micrometastases and small disease deposits. The practical reality, however, is that Tb-161 is only as scalable as its precursor target material: enriched Gadolinium-160 (Gd-160). China Isotope Development Co.,Ltd ,as a emerging Isotope supplier, was supplying Gadolinium-160 (Gd-160) to serve Researches & Institues step by step , gaining their trust ranging from its quality / price / delivery. Today, I want to guide you through the story of one such material: Gadolinium-160 (Gd-160). It is a stable, non-radioactive isotope, yet it stands as the essential starting point for producing one of the most promising cancer-fighting agents in modern radiotherapy: Terbium-161 (Tb-161).
Understanding the Foundation: A World of Isotopes
Before we delve into the specifics of Gd-160, it is crucial to grasp the concept of an isotope. From a nuclear scientist’s perspective, the identity of an element is defined by the number of protons in its atomic nucleus. For example, any atom with 65 protons is, by definition, a Gadolinium atom. However, the number of neutrons in that nucleus can vary. Atoms of the same element with different numbers of neutrons are called isotopes.
Some isotopes are “stable,” meaning their nucleus is in a balanced, non-decaying state. Others are “radioactive” (or “radionuclides”), possessing an unstable nucleus that releases energy in the form of radiation to transform into a more stable state. It is this very property of radioactive decay that we harness in nuclear medicine for both diagnosing and treating diseases like cancer.
Gadolinium: More Than Just an MRI Contrast Agent
For many in the medical community, the name “Gadolinium” is synonymous with MRI contrast agents. Indeed, certain gadolinium-based compounds are invaluable for enhancing the clarity of magnetic resonance imaging. However, this is only one facet of this versatile rare earth element. From a nuclear standpoint, the true potential lies within its individual isotopes.
Natural gadolinium is a mixture of several isotopes, two of which, Gd-155 and Gd-157, are famous for having extraordinarily high “neutron capture cross-sections.” This term simply describes their incredible ability to absorb thermal neutrons, making them useful as control rod materials in nuclear reactors.
Our focus today, however, is on a different, less abundant stable isotope: Gadolinium-160. While its neutron absorption capability is more modest compared to its siblings, its value is not in what it absorbs, but in what it becomes.
The Star of the Show: Gadolinium-160 (Gd-160)
Gadolinium-160 is a naturally occurring stable isotope, comprising about 21.86% of natural gadolinium. It has 65 protons and 96 neutrons, a combination that results in a stable nucleus. On its own, Gd-160 is unremarkable in a medical context. Its profound importance is realized only when we place it in the intense environment of a nuclear reactor. It is here that Gd-160 serves as the perfect “target material” for a process of nuclear alchemy that is revolutionizing cancer therapy.
The Core Process: From Stable Gd-160 to Therapeutic Tb-161
The transformation of Gd-160 into the medically invaluable Tb-161 is a two-step process, elegant in its physics and profound in its implications.
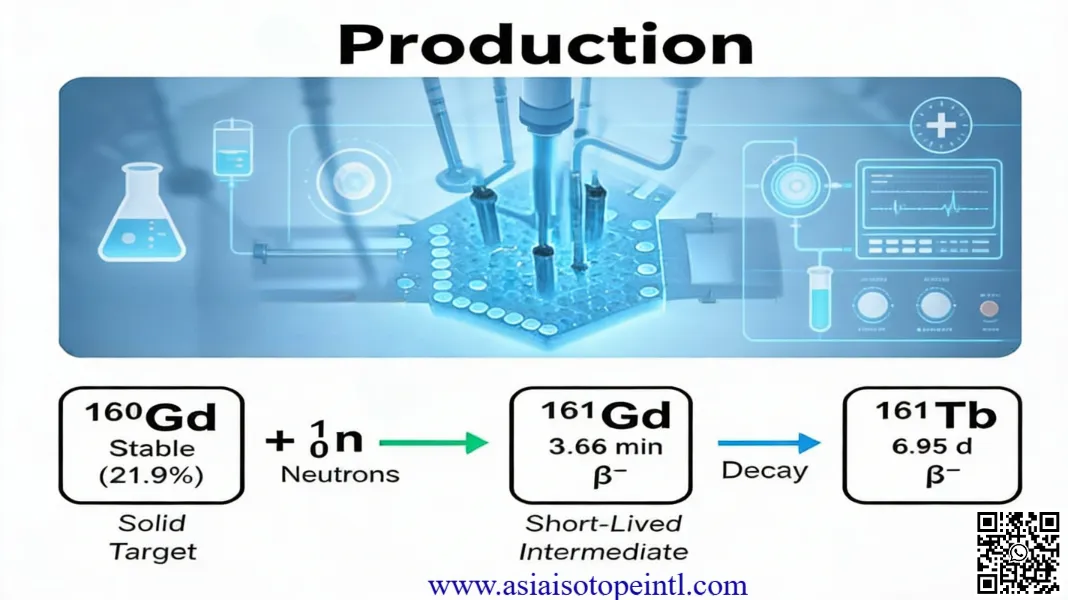
- Step 1: Neutron Capture. The process begins by taking highly enriched Gd-160—meaning the material has been processed to contain a much higher percentage of Gd-160 than found in nature—and placing it inside a nuclear reactor with a high flux of thermal neutrons. When a Gd-160 nucleus captures a neutron, it doesn’t split; instead, it transforms into a heavier isotope of the same element: Gadolinium-161 (Gd-161). This reaction is written as Gd-160(n,γ)Gd-161.
- Step 2: Beta Decay. The newly formed Gd-161 is radioactive, but its existence is fleeting. It has a very short half-life of about 3.66 minutes. It rapidly undergoes a process called beta-minus decay, where a neutron in its nucleus converts into a proton, releasing a beta particle (a high-energy electron) in the process. This transformation changes the fundamental identity of the atom. By gaining a proton, the atom with 65 protons (Gadolinium) becomes an atom with 66 protons: Terbium. Specifically, it becomes Terbium-161 (Tb-161).
Because Tb-161 is a different element from the original gadolinium target, it can be chemically separated to a very high purity, a state we refer to as “no-carrier-added.” This purity is absolutely essential for medical applications. This indirect production method is the gold standard for generating clinical-grade Tb-161.
Terbium-161: The “Swiss Army Knife” of Cancer-Fighting Radionuclides
So, why go through all this trouble to produce Tb-161? The answer lies in its unique and powerful decay properties, which make it an almost ideal radionuclide for a strategy known as “theranostics.”
Theranostics is a portmanteau of “therapy” and “diagnostics.” It refers to using a single agent that can both visualize a tumor (diagnose) and deliver a therapeutic dose of radiation to it (therapy). Tb-161 excels at this due to the cocktail of radiation it emits as it decays.
With a clinically convenient half-life of approximately 6.9 days, Tb-161 decays to stable Dysprosium-161. During this decay, it releases:
- Beta (β⁻) Particles: These are the primary therapeutic workhorses. They are electrons that travel a few millimeters in tissue, delivering a lethal dose of radiation to the tumor mass and nearby cancer cells.
- Gamma (γ) Rays: Tb-161 emits low-energy gamma rays that can exit the body and be detected by a SPECT (Single Photon Emission Computed Tomography) camera. This allows doctors to see exactly where the radiopharmaceutical has accumulated, confirming that it has reached the tumor and not healthy organs.
- Auger and Conversion Electrons: This is what truly sets Tb-161 apart and generates immense excitement in the field. In addition to beta particles, Tb-161 emits a significant shower of very low-energy electrons called Auger and conversion electrons. These electrons travel extremely short distances—on the scale of nanometers to micrometers, less than the width of a single cell.
This combination makes Tb-161 a multi-pronged weapon. The beta particles treat the bulk of the tumor, while the high-density, short-range Auger electrons are exceptionally effective at destroying single cancer cells and microscopic clusters of cells (micrometastases). It is these micrometastases that are often responsible for cancer recurrence after initial treatment, and they are notoriously difficult to eliminate with conventional therapies.
Clinical Significance: The Power of Targeted Radiotherapy
Producing Tb-161 is only half the story. To be effective, it must be delivered specifically to cancer cells while sparing healthy tissue. This is achieved through Targeted Radionuclide Therapy (TRT).
In TRT, the Tb-161 atom is attached to a “targeting molecule” using a chemical linker called a chelator. This targeting molecule is designed to seek out and bind to specific receptors that are overexpressed on the surface of cancer cells.
Two of the most prominent examples currently in clinical trials are:
- Prostate Cancer: The targeting molecule is a ligand like PSMA-617 or PSMA-I&T, which binds to the Prostate-Specific Membrane Antigen (PSMA) found on most prostate cancer cells. Clinical studies are exploring Tb-161-PSMA agents as a potentially more powerful alternative to the already successful Lutetium-177 (Lu-177) PSMA therapy.
- Neuroendocrine Tumors (NETs): The targeting molecule is a peptide analogue (like DOTATATE or DOTA-LM3) that binds to somatostatin receptors (SSTRs) on NET cells.
Once injected into the patient, this complete package—the radiopharmaceutical—travels through the bloodstream. The targeting molecule acts like a guided missile, homing in on the cancer cells. Once bound, the Tb-161 delivers its potent radiation payload directly to the tumor site. The Auger electrons are particularly devastating here, as their high-energy deposition in a tiny volume can cause complex, irreparable damage to the cancer cell’s DNA.
Preclinical and early clinical data have been incredibly promising, suggesting that Tb-161 can deliver a higher therapeutic dose to tumor cells—especially small ones—compared to Lu-177, a similar and widely used therapeutic radionuclide. This enhanced efficacy against micrometastases could be the key to improving long-term outcomes for patients and preventing disease relapse.
The Production Challenge: Why Enriched Gd-160 is a Strategic Asset
The pathway from Gd-160 to Tb-161 is elegant, but it is not without significant logistical and technical challenges. The most critical bottleneck is the availability of the starting material: highly enriched Gadolinium-160.
Natural gadolinium contains less than 22% Gd-160. Using natural gadolinium as a target in a reactor would be inefficient and would produce a host of unwanted isotopic impurities. To achieve the high specific activity and purity required for medicine, the starting material must be “enriched” to over 97.5% Gd-160.
Isotope enrichment is a technologically demanding and expensive process. It involves separating isotopes that have nearly identical chemical properties and differ only slightly in mass. Technologies like electromagnetic isotope separation are used, but they require specialized equipment and expertise. Furthermore, gadolinium itself presents unique challenges, as it requires extremely high temperatures to vaporize for the separation process.
Because of these difficulties, the global supply of highly enriched Gd-160 is limited. This makes it a strategic resource, the control of which is fundamental to the entire supply chain of Tb-161. Research institutions and commercial producers, such as the Paul Scherrer Institute (PSI) in Switzerland and companies like ITM, are making significant investments to scale up both Gd-160 enrichment and Tb-161 production to meet the anticipated clinical demand.
The Future Outlook: A New Era in Precision Oncology
As an isotope specialist who has tracked this field for my entire career, the trajectory of Gd-160 and Tb-161 is one of the most exciting developments I have witnessed. We are on the cusp of a new era in precision oncology. Phase 1 and 2 clinical trials for Tb-161-based radiopharmaceuticals are underway for prostate cancer and neuroendocrine tumors, with promising early results.
The journey from a stable, unassuming isotope like Gadolinium-160 to a cutting-edge, cancer-destroying agent like Terbium-161 is a testament to the power of nuclear science. It highlights a critical, often unseen, supply chain: from the complex physics of isotope enrichment and reactor irradiation to the sophisticated chemistry of radiolabeling and, finally, to the patient’s bedside.
Gadolinium-160 is not merely a precursor; it is the foundational key that unlocks the therapeutic potential of Terbium-161. As we continue to refine its production and expand its clinical applications, this quiet, stable isotope will play an increasingly loud and vital role in our fight against cancer.
Would you like a deeper dive into any specific technical parameters or applications?
As an industry leader focused in isotope products, our goal is to support our customers by keeping them at the forefront of their industries. We’re here to help with any questions you might have so you can transform your ideas into reality, and tackle those big science challenges.
Get free consultant, our experts are ready to serve.
(Follow up our update articles on www.asiaisotopeintl.com or send your comments to tao.hu@asiaisotope.com for further communications)